赵云
【摘要】目的 探讨评价吴茱萸穴位贴敷联合双足中药熏洗对胸痹心痛病气虚血瘀证患者的临床疗效。方法 选取我院心血管内科2018年01月~2019年12月间52例胸痹心痛病气虚血瘀证患者,随机均分为对照组和观察组各26例。对照组接受活血化瘀中西医药物治疗及护理,观察组在对照组药物治疗基础上配合吴茱萸子午流注穴位热敷联合双足中药熏洗中医护理干预。干预2周,对比两组心功能和血压控制情况、治疗有效率、心绞痛发作次数及睡眠质量。结果 干预后,观察组心功能改善程度明显优于对照组,表现为左室射血分数(LVEF)明显高于本组干预前及对照组干预后,差异有统计学意义(P<0.05),观察组左室舒张末期内径(LVEDD)小于本组干预前及对照组干预后监测水平;两组血压干预后均明显低于干预前,且观察组下降水平较对照组更为明显,差异有统计学意义(P<0.05);观察组总有效率明显高于对照组,观察组心绞痛发作次数及匹兹堡睡眠质量指数PSQI評分明显低于对照组,差异有统计学意义(P<0.05)。结论 吴茱萸穴位贴敷联合双足中药熏洗中医护技术应用,能明显缓解胸痹心痛病气虚血瘀证患者的临床症状,患者心功能、血压水平及睡眠质量明显改善,心绞痛发作次数明显减少,效果显著。
【关键词】胸痹心痛病;穴位贴敷;中药熏洗;心功能;血压;睡眠质量
【中图分类号】R245.9 【文献标识码】A 【文章编号】ISSN.2095.6681.2020.6..03
【Abstract】Objective To evaluate and evaluate the clinical efficacy of acupoint application of Evodia rutaecarpa combined with Chinese foot fumigation and washing on qi deficiency and blood stasis syndrome of chest pain and heartache.Methods From January 2018 to December 2019,52 patients with chest palsy and heartache disease with Qi deficiency and blood stasis syndrome were randomly selected and randomly divided into the control group and the observation group with 26 cases each. The control group received treatment and nursing of traditional Chinese and western medicines for promoting blood circulation and removing blood stasis. The observation group based on the drug treatment of the control group cooperated with rutaecarpus meridian injection hot acupoints combined with traditional Chinese medicine fumigation and washing with two feet of Chinese medicine. After 2 weeks of intervention, the heart function and blood pressure control, treatment efficiency, number of angina pectoris episodes, and sleep quality were compared between the two groups.Results After the intervention,the improvement of cardiac function in the observation group was significantly better than that in the control group,and the left ventricular ejection fraction (LVEF) was significantly higher than that in this group and before the control group (P<0.05).(LVEDD) is lower than the monitoring level before and after intervention in this group; blood pressure after intervention in both groups is significantly lower than before intervention, and the level of decline in the observation group is more significant than that in the control group (P<0.05);the total effective rate in the observation group It was significantly higher than the control group.The number of angina pectoris episodes and the Pittsburgh Sleep Quality Index PSQI score in the observation group were significantly lower than those in the control group (P<0.05).Conclusion The application of acupoint application of Evodia rutaecarpa combined with traditional Chinese medicine fumigation and washing with biped feet can obviously alleviate the clinical symptoms of patients with chest pain and heartache,qi deficiency and blood stasis syndrome,patients' cardiac function,blood pressure level and sleep quality are significantly improved,and the number of angina pectoris attacks is significantly reduced.Significantly.
【Key words】Chest pain and heartache;Acupoint application;Chinese medicine fumigation;Heart function;Blood pressure;Sleep quality
胸痹心痛病是中医学中较为多见的以胸膺部窒塞疼痛为主的一种痹证,与现代西医学冠心病、心绞痛症状类同。其中气虚血瘀证病因均由心气不足为本,血脉营运受阻以致淤血痰浊内停为标,其临床主要症状以胸闷、胸痛、心悸气短、乏力等为主,疾病程度严重者卧床时症状更为显普,严重影响患者生活质量[1]。近年来,临床对胸痹心痛病采取中西医结合治疗已取得了较大的进展,中医护理方案也得到了很好的作用验证[2]。本文将我院运用吴茱萸穴位贴敷联合双足中药熏洗对胸痹心痛病气虚血瘀证患者的临床疗效进行总结并报道如下。
1 资料和方法
1.1 一般资料
选取连云港市灌云县中医院2018年01月~2019年12月52例胸痹心痛病气虚血瘀证患者,随机均分为对照组和观察组各26例。纳入标准:(1)心绞痛病史超过4个月,诊断明确,第一诊断为胸痹心痛(气虚血瘀证),符合《中医内科常见病诊疗指南》与《中药新药临床研究指导原则》 [3];(2)西医诊断冠心病稳定型劳累性心绞痛,符合WHO制定的《缺血性心脏病的命名及诊断标准》和《高血压处理指南》诊断标准[4]。排除皮肤过敏及破损、合并糖尿病及恶性高血压患者。对照组男14例,女12例,年龄49~88岁,平均(68.52±5.34)岁;病程5~30年,平均(15.25±3.32)年;心功能分级:Ⅰ~Ⅱ级11例,Ⅲ~Ⅳ级15例;高血压分级:1级10例,2级9例,3级5例,单纯收缩期高血压2例。观察组男15例,女11例,年龄50~89岁,平均(69.13±6.12)岁;病程6~32年,平均(16.41±3.38)年;心功能分级:Ⅰ~Ⅱ级10例,Ⅲ~Ⅳ级16例;高血压分级:1级11例,2级8例,3级4例,单纯收缩期高血压3例。两组一般资料比较无明显差异,差异无统计学意义(P>0.05)。
1.2 方法
1.2.1 对照组
实施活血化瘀、调脂利尿及改善心肌等中西医药物治疗及常规护理:(1)药物治疗:常用酒石酸美托洛尔片25 mg口服,2次/日。厄贝沙坦氢氯噻嗪片150 mg口服,1次/日,瑞舒伐他汀钙片10 mg口服,1次/晚,阿司匹林肠溶片0.1 mg,口服,1次/日,麝香保心丸2粒口服,tid;红花黄色素2支加入0.9%氯化钠注射液100 mL,静脉滴注,1次/日。配合中药颗粒剂一日一剂口服。(2)护理措施:为患者提供安静、舒适的休息环境,做好生活护理和心理护理,确保患者情绪平静、舒适,消除患者紧张、恐惧、焦虑的心理,对于睡眠欠佳者必要时可遵医嘱给予助眠药物口服。指导患者进食清淡易消化富含纤维素的膳食,适度运动,多吃新鲜蔬菜和水果以促进肠蠕动,预防便秘,便秘严重者必要时给予缓泻剂[5]。
1.2.2 观察组
在对照组药物治疗基础上增加吴茱萸中药穴位贴敷联合双足熏洗中医护理干预措施:(1)吴茱萸中药穴位贴敷:选取院内制剂吴茱萸穴位贴敷疗法,取中药吴茱萸25 g研末,以甘油、白醋调制而成穴位贴,于每日上午9~13时选双足涌泉穴、足三里和大椎穴位行外贴敷,贴敷时间6 h,1次/日,2周为一疗程。(3)双足中药熏洗:于患者每晚睡前2小时戌时(19点~21点)实施,取太子参15 g,红花25 g,丹参50 g,制草乌25 g,生甘草30 g,制川乌25 g,川芎25 g,桂枝25 g,诸药加水1000 mL浸泡30 min,煎煮30 min取汁倒入足浴盆,患者双足置于盆沿熏蒸,待水温降至45℃~55℃时双足放入盆内泡足40 min,2周为一疗程。
1.3 观察指标
(1)通过心脏彩超检查的左室射血分数(LVEF)和左室舒张末期末径(LVEDD)结果了解患者心功能指标 [6]。(2)参照中医证候积分疗效率评价患者中医临床疗效,有效率=显效率+有效率。中医证候积分减少≥70%为显效,临床症状基本消失,心功能显著改善;积分减少在30%~70%为有效,临床症状有所减轻,心功能改善明显;积分减少<30%为无效,心功能及临床症状无改善[7]。(3)通过收缩压和舒张压水平变化判断有效血压控制情况;(4)运用匹兹堡睡眠质量指数量表(PSQI)评价患者睡眠质量,包括睡眠质量、睡眠障碍、日间功能、入睡时间、睡眠时间5个项目,每项目0~3分,总分0~21分,分数越高代表睡眠质量越差[8]。
1.4 统计学方法
采用SPSS 19.0统计軟件数据分析,计数资料以[n(%)]表示,采用x2 检验,计量资料采用均数±标准差(x±s)表示,采用t检验,P<0.05表示差异有统计学意义。
2 结 果
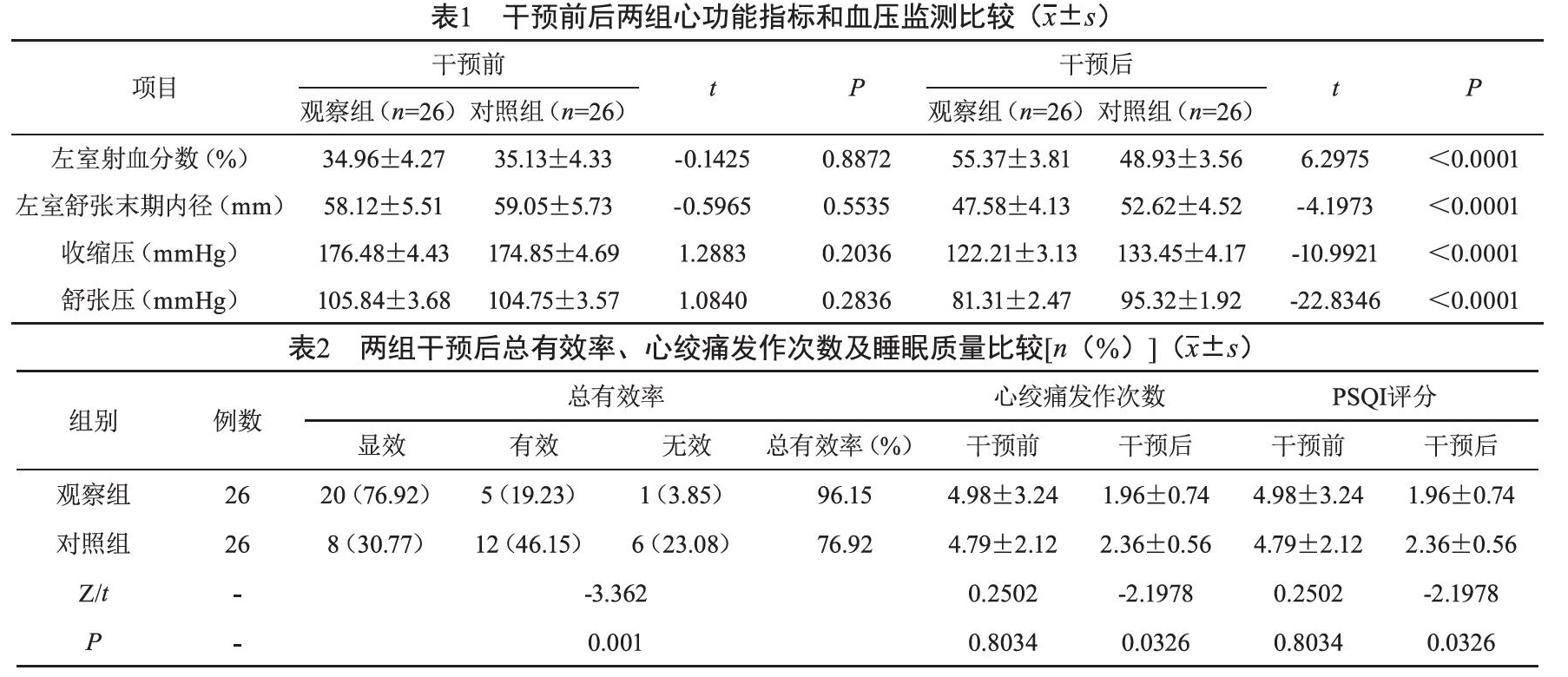
2.1 干预前后两组心功能指标和血压监测比较
干预后,观察组心功能改善程度明显优于对照组,表现为左室射血分数(LVEF)左室射血分数明显高于本组干预前及对照组干预后,差异有统计学意义(P<0.05),观察组左室舒张末期内径(LVEDD)小于本组干预前及对照组干预后监测水平;两组血压干预后均明显低于干预前,且观察组下降水平较对照组更为明显,差异有统计学意义(P<0.05)。(见表1)。
2.2 两组干预后总有效率、心绞痛发作次数及睡眠质量比
较干预后,观察组总有效率明显高于对照组,观察组心绞痛发作次数及匹兹堡睡眠质量指数PSQI评分明显低于对照组,差异有统计学意义(P<0.05)。见表2
3 讨 论
胸痹心痛病的病机多因情志波动、饮食不当、劳倦过度及寒邪内侵等诱发,引起冠脉血液循坏障碍、心肌供血不足,从而导致发病。其中气虚血瘀证型者多伴有胸部不适、心神不宁、血色晦暗等症状,治则宜采取宣痹通阳、益气活血、通阳化痰疗法[9]。
- 钢琴演奏中的触键技巧对音色效果的影响探究
- 浅谈如何进行音乐作品赏析
- 声乐表演艺术的审美体现分析
- “练声”不如“练耳”
- 轻拂休止符的神秘面纱
- 通过二声部训练培养多声思维能力
- 钢琴演奏中的状态调整
- 钢琴教学中演奏呼吸的规律分析
- 从唐前期敦煌莫高窟药师经变图浅究药师经变乐队编制
- 晋察冀抗日根据地《穷人乐》的创作及影响
- 浅析罗西尼歌剧对美声唱法的影响
- 唐代音乐传承观念的能动性研究
- 琵琶曲《普庵咒》源流考
- 浅谈音乐剧的文化价值
- 浅析舞蹈中“情”与“理”
- 浅谈舞蹈编创问题
- 弘扬民族文化 聆听民乐经典
- 论艺术惠民工程对传承中华民族传统文化的重要性
- 音乐心理学视野下的音乐学习路径研究
- 论双人舞《振翅重飞》的情感表达
- 从雄安新区文化建设角度谈传统音乐教育与文化传承发展的对接
- 舞蹈编导的创作思想及结构分析
- 基层文化馆文艺辅导及人才建设探究
- 由龙江剧《百米河边》分析龙江剧的发展、特征和传承
- 论古筝音乐在影视作品中的运用与结合
- overshortness
- overshortnesses
- overshot
- overshrank
- overshrink
- overshrinking
- overshrinks
- overshroud
- overshrunk
- overshrunken
- oversight
- oversights
- oversilence
- oversilences
- oversilent
- oversilently
- oversilentness
- oversilentnesses
- oversimpleness
- oversimplenesses
- oversimplicities
- oversimplicity
- oversimplification
- oversimplifications
- oversimplified
- 繁月无
- 繁木
- 繁本
- 繁朵
- 繁杂
- 繁杂1
- 繁杂2
- 繁杂啰嗦
- 繁杂忙碌而不见成绩,无所建树
- 繁杂急迫的事务
- 繁杂污浊
- 繁杂混乱
- 繁杂琐碎
- 繁杂的事务
- 繁杂的思绪
- 繁杂的政事
- 繁杂的枝条
- 繁杂紊乱
- 繁杂累赘的词句
- 繁杂纷乱
- 繁杂纷扰
- 繁杂而劳苦的事
- 繁杂苛细
- 繁杂辛苦的样子
- 繁条