柯新

[摘要]目的 分析经伤椎椎弓根植骨联合后路短节段椎弓根钉内固定(SSPI)治疗胸腰椎爆裂性骨折(TBF)的临床效果。方法 选取2015年6月~2017年10月我院收治的53例TBF患者为研究对象,均采用SSPI治疗,按照椎体内植骨与否分为两组。其中A组(28例)单纯采用SSPI治疗,B组(25例)采用经伤椎椎弓根植骨联合SSPI治疗。比较两组手术时间、术中出血量、术后引流量,术前、术后1周、末次随访时伤椎椎体前缘高度比及后凸Cobb角,术后神经功能ASIA分级改善情况,术后视觉模拟量表(VAS)评分。结果 两组手术时间、术中出血量、术后引流量比较,差异无统计学意义(P>0.05)。术前、术后1周,两组伤椎椎体前缘高度比及后凸Cobb角比较,差异无统计学意义(P>0.05),但末次随访时B组伤椎椎体前缘高度比大于A组,椎体后凸Cobb角小于A组,差异有统计学意义(P<0.05)。B组术后神经功能ASIA分级改善情况优于A組,VAS评分低于A组,差异均有统计学意义(P<0.05)。结论 经伤椎椎弓根植骨联合SSPI治疗TBF能有效恢复伤椎高度,矫正伤椎后凸畸形,缓解疼痛,有助于神经功能恢复,是一种有效的治疗方法。
[关键词]胸腰椎;爆裂性骨折;经椎弓根;植骨;椎弓根钉;内固定
[中图分类号] R687.3? ? ? ? ? [文献标识码] A? ? ? ? ? [文章编号] 1674-4721(2019)10(a)-0133-04
[Abstract] Objective To observe the effect on thoracolumbar burst fractures(TBF) treated by posterior bone graft through vertebral pedicle and short-segmental pedicle screw internal fixation (SSPI). Methods All 53 cases of TBF treated by SSPI in our hospital from June 2015 to October 2017 were enrolled. All patients divided into group A (28 cases), group B (25 cases) according to with/without bone graft through vertebral pedicle. Group A was treated with SSPI, and group B was treated with bone graft through vertebral pedicle and SSPI. The operation time, intraoperative blood loss, and postoperative drainage were recorded. The ratio of anterior vertebral height and kyphosis Cobb angle were recorded before, 1 week after operation and at the last follow-up. The postoperative neurological function of the two groups was evaluated according to ASIA classification. The postoperative visual analogue scale (VAS) scores of the two groups were compared. Results There were no significant difference in the operation time, intraoperative blood loss, postoperative drainage, one week before and after operation ratio of anterior vertebral height and Cobb angle between the two groups (P>0.05). However, at the last follow-up, the ratio of anterior vertebral height was higher and Cobb angle was smaller in group B than those of group A, and the differences were statistically significant (P<0.05). The improvement of postoperative neurological ASIA grading was better and the VAS score was lower in group B than those in group A, and the differences were statistically significant (P<0.05). Conclusion Treatment of TBF with bone graft through vertebral pedicle and SSPI by posterior approach can effectively restore the height of the injured vertebrae, correct the kyphosis deformity, relieve pain and promote the recovery of nerve function, which is an effective method.
3讨论
TBF多因车祸、高坠等引起。椎体受到轴向暴力冲击时发生机械性破坏,高能纵向载荷使椎体前中柱压缩并向四周迸裂,椎体失稳,移行骨折块突入椎管压迫脊髓使椎管压力增加,引起严重神经症状,使患者丧失生活自理能力,生活质量严重降低[6-7]。骨折诱因除与轴向载荷的力度、方向有关外,与该部位解剖结构也有关联。①缺乏胸廓、肋骨保护[8];②该部位为胸腰椎力学特性转换区域,易导致局部应力集中,椎体易损伤[9];③该部位关节突关节面走向发生变化,易受轴向旋转负荷的破坏[10]。
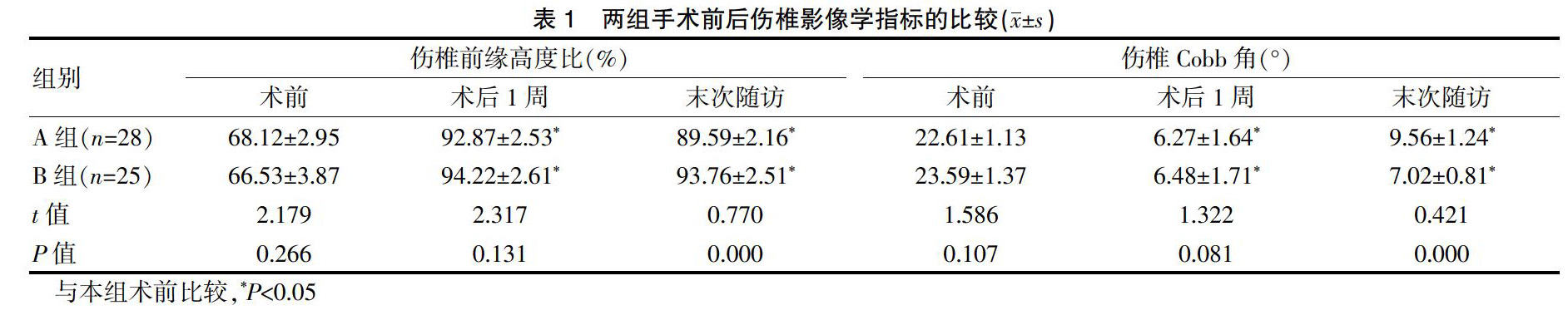
临床多采用手术治疗TBF,SSPI即是常用术式之一。其特点:①骨折伤及终板使椎间盘髓核被挤入椎体内,椎体高度、椎间隙丢失引起后凸畸形,伤椎置钉能支撑椎体即刻恢复伤椎前缘高度,迅速增加椎间隙,矫正畸形[11]。本研究两组术后伤椎前缘高度比较术前均增加、后凸Cobb角较术前减小即与上述因素有关。②术中可打压向后移行的骨折块,实现椎管直接减压。③椎间隙高度增加后通过后纵韧带的张力可对椎管间接减压。因而术后可迅速缓解疼痛,促进神经功能恢复,本研究两组术后神经功能较术前改善,VAS评分较术降低即与上述因素有关。
内固定术后有松动、断裂、复位丢失等并发症。原因:①置钉虽能撑开椎体,但椎体呈中空蛋样,在骨折修复时伤椎体内脂肪组织会进行替代,椎体强度丢失,抗压能力减弱,术后出现复位丢失或进展性后凸畸形[12]。而椎体不稳也不利于骨折愈合,可能导致内固定失败。②三柱理论认为椎体前中柱起着主要的支撑作用,是维持脊柱稳定的关键之一[13]。后路椎管减压对椎体中柱结构进一步造成破坏,而螺钉对椎体前中柱支撑力也相对有限,导致椎体前中柱支撑不足,术后椎体后凸畸形的可能性增大[14]。
为避免上述不足,B组对伤椎植骨,其优点如下。①可有效解决伤椎空蛋样问题,恢复伤椎的强度和刚度,恢复前中柱支撑作用,有效避免术后复位丢失。②给伤椎骨折愈合及神经损伤修复提供稳定的力学环境,有利于骨折愈合和神经修复[15]。B组术后随访时植骨均骨性融合,末次随访时椎体高度维持满意,未出现内固定失败等并发症。
综上所述,经伤椎植骨结合SSPI治疗TBF,能有效恢复椎体高度,矫正后凸畸形,缓解疼痛并促进神经功能恢复,且术后可长期维持复位效果,是一种有效的治疗方法。
[参考文献]
[1]Li B,Sun C,Zhao C,et al.Epidemiological profile of thoracolumbar fracture (TLF) over a period of 10 years in Tianjin,China[J].J Spinal Cord Med,201,42(2):178-183.
[2]梁晓,邓信昌,罗登熙,等.经椎弓根植骨联合椎弓根钉内固定治疗胸腰段椎体爆裂骨折[J].泰山医学院学报,2018, 39(7):779-781.
[3]李益明,夏计划,姜效韦,等.经椎弓根植骨联合椎弓根钉内固定治疗胸腰段椎体爆裂骨折的疗效分析[J].中国骨与关节损伤杂,2017,32(7):734-736.
[4]冯晰旻,赵旭鹏,李哲,等.后路伤椎单侧置钉并椎体植骨治疗胸腰椎骨折的远期效果[J].中国骨与关节损伤杂志,2012,27(3):232-233.
[5]罗肖,陈敬忠,陈铖.短节段椎弓根钉固定手术治疗脊柱骨折的效果及对患者脊髓功能影响情况研究[J].创伤外科杂志,2018,20(7):536-539.
[6]张景林,高洪辉,刘晓龙,等.经伤椎椎弓根植骨置钉后路内固定治疗胸腰椎爆裂性骨折[J].创伤外科杂志,2015, 17(1):39-42.
[7]侯磊,郭开今,吴继彬.短节段内固定结合经椎弓根椎体内植骨治疗胸腰椎爆裂性骨折[J].中国临床研究,2018, 31(6):105-108.
[8]梁朝革,于荣华.胸腰椎爆裂性骨折治疗[J].创伤外科杂志,2018,20(4):84-87.
[9]付裕,霍洪军,杨学军,等.伤椎后路椎弓根螺钉置入并椎体内植骨重建胸腰椎椎体的高度[J].中国组织工程研究与临床康复,2011,15(43):8075-8078.
[10]苏新磊,张桂莲,杨忠奎,等.经伤椎与跨伤椎椎弓根短节段内固定治疗胸腰椎爆裂性骨折的临床疗效对照研究[J].广东医学,2018,39(19):68-72.
[11]尹偉,张波,卫永鲲,等.经椎弓根伤椎植骨结合短节段椎弓根钉内固定治疗胸腰椎骨折的临床效果分析[J].颈腰痛杂志,2018,39(3):119-120.
[12]胡海刚,谭伦,林旭,等.经伤椎椎弓根植骨置钉后路复位内固定术治疗胸腰椎骨折[J].中国脊柱脊髓杂志,2011, 21(8):663-668.
[13]董福龙,宋旆文,葛鹏,等.单一后路减压联合前-中柱重建治疗严重胸腰椎爆裂性骨折[J].安徽医科大学学报,2017,52(8):137-141.
[14]曹众,王敏,孟庆奇.经椎弓根植骨与非植骨内固定治疗胸腰椎爆裂骨折疗效对比[J].实用医学杂志,2018,34(16):2692-2695.
[15]蔡亮,熊东波,付江明,等.经伤椎椎弓根植骨联合后路伤椎椎弓根内固定治疗胸腰椎爆裂性骨折[J].中外健康文摘,2011,8(18):46-49.
(收稿日期:2019-02-21? 本文编辑:崔建中)
- 癫痫患儿家庭焦虑情绪的调查研究
- 微生物检验标本不合格原因分析及质量控制对策研究
- 厄贝沙坦+氨氯地平治疗原发性高血压的效果分析
- 关于小儿手足口病的预防和控制对策探讨
- 探讨血液病进行血液形态学检验、骨髓活检、免疫分型和细胞遗传学联合检查特点
- 分析高原地区老年人慢性肺心病急性加重期心律失常的临床特点
- 老年颈肩腰腿痛的针灸推拿防治策略分析
- 哮喘与脑卒中发生风险的Meta分析
- 微生态制剂在溃疡性结肠炎患者的疗效分析
- 乙肝病毒性肝炎患者两对半临床医学检验分析
- 尿沉渣镜检法与尿干化学法在尿液检验中的相关性探讨
- 超声心动图诊断冠心病节段性室壁运动异常的临床应用价值分析
- 基于药品集中采购的药品购销模式研究
- 2016-2018年我院住院患者抗菌药物使用情况分析
- 中医综合疗法联合特色护理治疗带状疱疹后遗痛的效果观察
- 新生儿重症呼吸衰竭患儿治疗中运用高频振荡通气的临床效果探讨
- 高频彩超在甲状腺占位性病变中的诊断价值
- 导致西药房处方调剂差错出现的原因及防范对策分析
- 奥林巴斯电子胃镜常见故障处理与维修探讨
- 超声远程会诊中的法律关系及探讨
- 基于血液标本采集对生化检验结果的影响分析
- 探讨有创呼吸机、无创呼吸机序贯治疗重症慢阻肺Ⅱ型呼吸衰竭的临床疗效
- 我国当前留守儿童心理问题分析及预防策略
- 腹腔镜手术与开腹手术治疗急性复杂性阑尾炎临床疗效比较分析
- 微生物检验在感染控制中的应用价值分析
- practised
- practise/practice
- practiser
- practises
- practise's
- practising
- practisingcertificate
- practising cerˌtificate
- practitioner
- practitioners
- pragmatic
- pragmaticalities
- pragmatically
- pragmaticalness
- pragmaticalnesses
- pragmatism
- pragmatisms
- pragmatist
- pragmatists
- prairie
- prairied
- prairielike
- prairies
- praisably
- praise
- 摆班
- 摆理
- 摆瓢
- 摆盘儿
- 摆知
- 摆砌末
- 摆碟子
- 摆簸
- 摆绺
- 摆缕
- 摆置
- 摆美人计
- 摆老
- 摆老资格
- 摆老资格,自以为了不起的样子
- 摆肉头阵
- 摆脱
- 摆脱世俗的高雅境界
- 摆脱了受压抑的境况,变得精神愉快
- 摆脱了坏伙伴的人,才可以谈前途
- 摆脱困厄或解除弊病的手段
- 摆脱困境
- 摆脱困境的日子已经为期不远
- 摆脱困境,彻底好转起来
- 摆脱困境,获得自由,进入广阔天地