王保群 刘军军 辛海 官笑梅 李君 王豪夫

[摘要] 目的 探討股腘动脉硬化闭塞症膝下动脉逆行开通的安全性和有效性。方法 收集2015—2016年在我院治疗的TASCⅡ C/D型股腘动脉硬化闭塞症病人,其中接受膝下动脉逆行腔内介入(REI)治疗者33例(REI组),常规经股动脉开通治疗者97例(TFA组),比较两组的技术成功率、手术并发症发生率、血管通畅率、保肢率。结果 REI组与TFA组的技术成功率分别为78.8%和90.2%。REI组与TFA组并发症发生率分别为9.1%和6.9%,差异无统计学意义(P>0.05)。术后平均随访19.8个月(1~30月),REI组和TFA组的一期通畅率术后1年时分别为48.4%和54.2%,术后2年时分别为29.4%和50.6%;REI组和TFA组的辅助一期通畅率术后1年时分别为63.1%和73.3%,术后2年时分别为36.3%和58.4%。TFA组一期通畅率和辅助一期通畅率相对较高,但差异均无统计学意义(P>0.05)。REI组术后1、2年时的保肢率分别为93.0%和87.5%,TFA组分别为100.0%和95.4%,两组保肢率比较差异无显著性(P>0.05)。结论 膝下动脉REI与常规经股动脉开通治疗TASCⅡ C/D型股腘动脉硬化闭塞症,随访期间血管通畅率相当,且远端穿刺部位并发症很少发生,因此REI可作为常规经股动脉入路开通失败后的补救治疗手段。
[关键词] 闭塞性动脉硬化;腘动脉;血管成形术;膝下动脉;治疗结果
[中图分类号] R654.3;R543.5[文献标志码] A[文章编号] 2096-5532(2021)01-0110-05
[ABSTRACT]ObjectiveTo investigate the safety and efficacy of infrageniculate retrograde arterial access in the treatment of femoropopliteal arteriosclerosis obliterans. MethodsA retrospective analysis was performed for the patients with TASC Ⅱ type C/D femoropopliteal arteriosclerosis obliterans who were treated in our hospital from 2015 to 2016, and among these patients, 33 underwent retrograde endovascular intervention (REI) (REI group) and 97 underwent conventional transfemoral access (TFA) (TFA group). The two groups were compared in terms of technical success rate, incidence rate of postoperative complications, vascular patency rate, and limb salvage rate.ResultsThe technical success rate was 78.8% in the REI group and 90.2% in the TFA group. The incidence rate of complications was 9.1% in the REI group and 6.9% in the TFA group, with no significant difference between the two groups (P>0.05). The mean follow-up time was 19.8 months (1-30 months) after surgery; at 1 year after surgery, the REI group had a primary patency rate of 48.4% and an assisted primary patency rate of 63.1%, and the TFA group had a primary patency rate was 54.2% and an assisted primary patency rate of 73.3%; at 2 years after surgery, the REI group had a primary patency rate of 29.4% and an assisted primary patency rate of 36.3%, and the TFA group had a primary patency rate was 50.6% and an assisted primary patency rate of 58.4%. The TFA group had slightly higher primary patency rate and assisted primary patency rate than the REI group (P>0.05). The REI group had a 1 year limb salvage rate of 93.0% and a 2 year limb salvage rate of 87.5%, and the TFA group had a 1 year limb salvage rate of 100.0% and a 2 year limb salvage rate of 95.4%, with no significant difference between the two groups (P>0.05). ConclusionIn the treatment of TASC Ⅱ type C/D femoropopliteal arteriosclerosis obliterans, infrageniculate arterial REI has a comparable vascular patency rate to TFA, with few complications at the distal site of puncture, and therefore, REI can be used as a remedial treatment after the failure of TFA.
[KEY WORDS]arteriosclerosis obliterans; popliteal artery; angioplasty; below-the-knee arteries; treatment outcome
TASCⅡ C/D型股腘動脉硬化闭塞症是较为严重的外周动脉疾病(PAD),有较高的发病率和死亡率,其临床特征为间歇性跛行、静息痛、缺血性溃疡或前足和足趾远端坏疽,在解剖上通常表现股动脉向膝下病变区段延伸的慢性完全闭塞(CTO)[1-2]。尽管腔内治疗器械和技术不断发展,但是仍有10%~20%的复杂CTO病人顺行开通失败,主要是由于在内膜下开通过程中无法跨越动脉闭塞段或无法重新返回真腔。在这些病人中,由于缺乏自体移植静脉,流出道较差或伴有严重的并发症,全身麻醉下的外科旁路手术很难施行[3],因而需要一种新的治疗手段对闭塞血管进行开通。以往的研究表明,通过膝下动脉逆行开通对于顺行开通失败的病人是一种可供选择的治疗方案[4-5],但文献中缺乏膝下动脉逆行开通和常规经股动脉开通治疗股腘动脉硬化闭塞症效果的比较。因此,本研究对这两种方式治疗股腘动脉闭塞症的短中期效果进行了比较。
1 资料和方法
1.1 一般资料
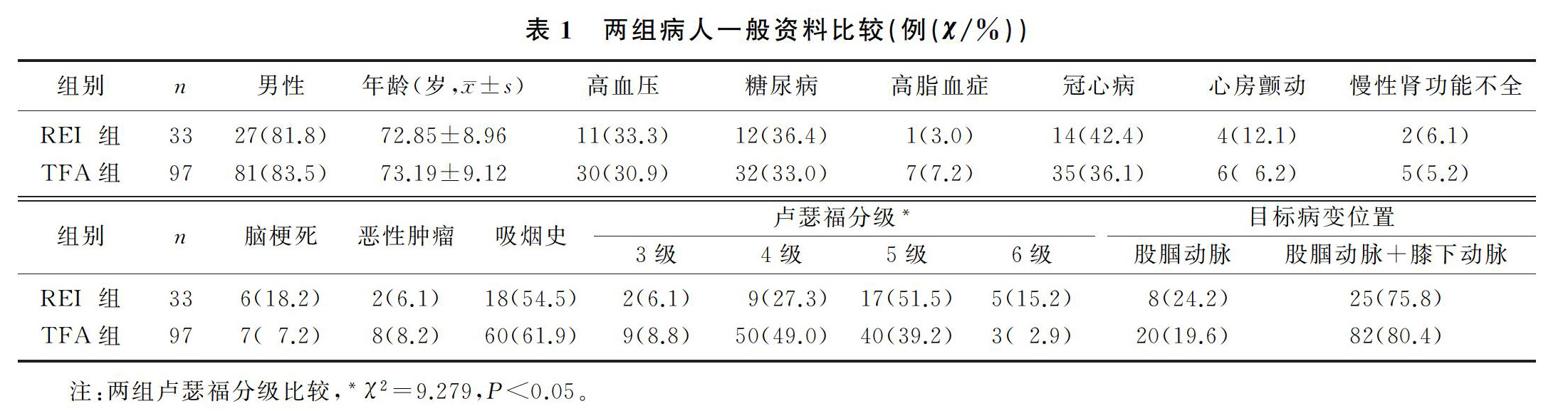
收集2015—2016年在青岛大学附属医院治疗的TASCⅡ C/D型股腘动脉硬化闭塞症病人,其中常规经股动脉顺行开通失败而接受膝下动脉逆行腔内介入(REI)治疗者33例(REI组),常规经股动脉开通治疗者97例(TFA组),所有手术均由我科医生完成。两组病人的基线资料比较,除卢瑟福分级差异有统计学意义(χ2=9.279,P<0.05)外,其余资料差异均无显著性(P>0.05)。见表1。
1.2 手术方法
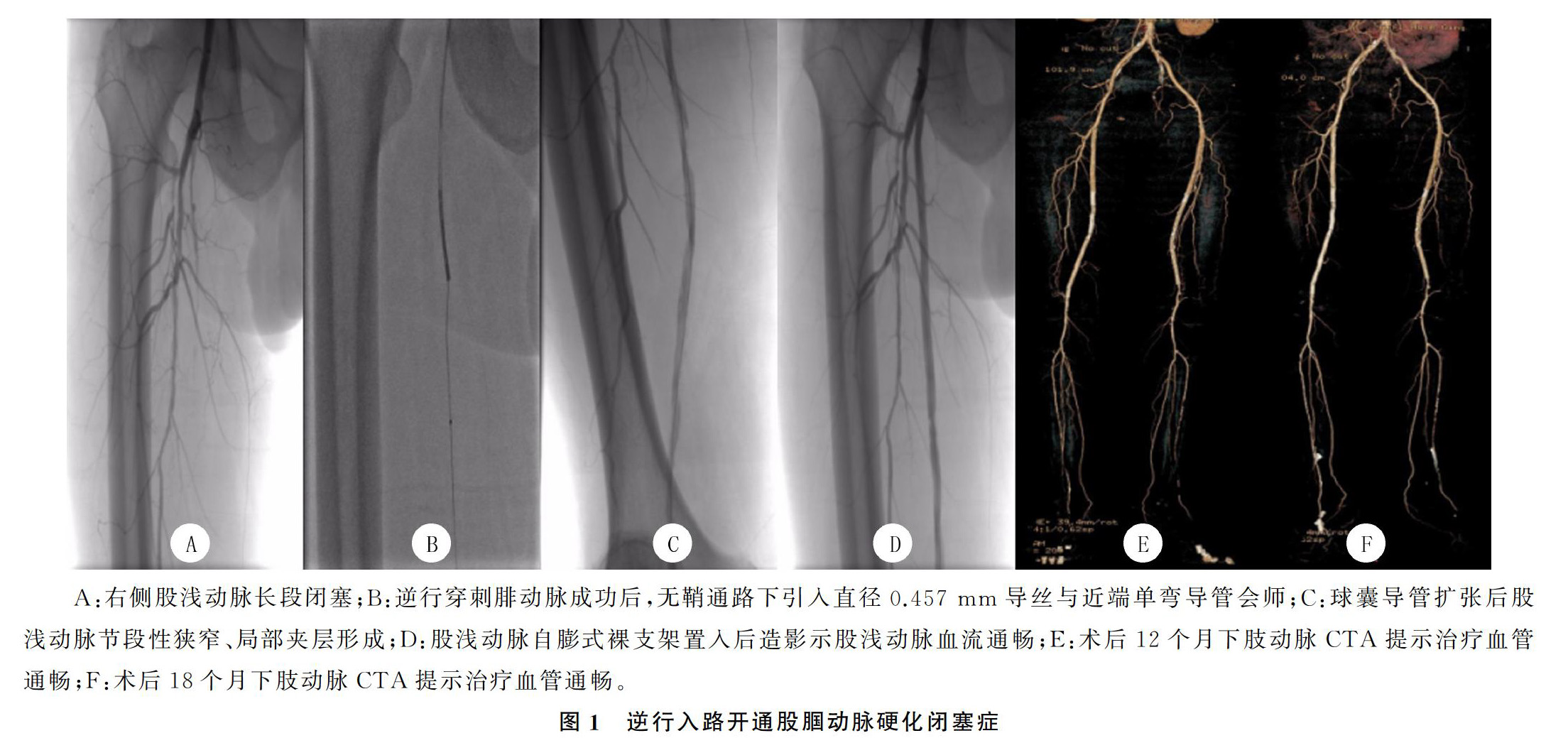
局麻下采用Seldinger技术穿刺同侧或者对侧股总动脉,穿刺成功之后置入5F导管鞘。静脉推注100 U/kg普通肝素,然后通过血管造影明确病变位置,根据所需选择合适的导丝及开通设备,使用标准的导管技术跨越股腘动脉闭塞段。反复开通闭塞段失败或无法返回真腔则启动REI,确定穿刺部位后在路图下选择病变程度最小的动脉段进行经皮穿刺。如果经皮穿刺失败,则取小切口直视下穿刺。通过使用4F微穿刺针套件(Cook),获得无鞘通路后引入直径0.457 mm导丝,球囊导管或4F单弯导管作为支撑导管在直径0.457 mm导丝上以“无鞘”方式推进,必要时置入4F导管鞘。一旦导丝配合导管逆行通过CTO重返近端动脉真腔,则将导丝从顺行导管鞘中引出,从而为顺行介入操作提供了工作轨道。在内膜下开通的情况下,如果逆行开通导丝在穿过CTO段后未能重新返回真腔,则采用“双球囊”技术扩张[6]。该技术是根据血管直径在顺行和逆行导丝上双向引入合适的球囊导管,避免使用直径过小的球囊导管,并以不同的角度检查两根球囊导管尖端相对接近的距离,两个球囊导管同时进行扩张撕裂内膜并将导丝定位在真腔中[7]。工作轨道建立后,立即撤出逆行导丝、导管,穿刺点处球囊贴附3~5 min,所有后续介入操作均在顺行入路进行[8]。最后,进行CT血管造影(CTA)以评估股腘动脉以及膝下流出道的通畅性。见图1。
1.3 疗效评价
比较两组的技术成功率、主要不良事件(MAE)发生率、手术并发症发生率、血管通畅率、保肢率和生存率等。技术成功及失败:技术成功定义为治疗结束后造影显示目标血管残余狭窄小于30%;技术失败定义为穿刺失败或无法完成血运重建而导致手术失败。MAE定义为病人死亡、非致死性急性心肌梗死、通过下肢动脉经皮腔内血管成形术(PTA)或外科旁路手术进行靶血管的反复血运重建或大截肢。血管通畅:一期通畅是指随访期间治疗段血管没有闭塞且再狭窄程度小于30%;辅助一期通畅是指需要一个辅助的干预来保持一期通畅或治疗一个显著的再狭窄。通过随访临床特征以及无创检查(踝肱指数测定、下肢动脉彩超)评估上述指标,必要时行下肢动脉CTA。在病人水平上分析生存率,在肢体水平上分析其他结果。
1.4 统计学方法
应用IBM SPSS Statistics 22软件进行统计分析。两组计数资料比较采用卡方检验,计量资料比较采用t检验;通过Kaplan-Meier曲线对通畅率、保肢率和生存率进行评估。P<0.05则认为差异有统计学意义。
2 结果
2.1 治疗方式
经股动脉顺行开通过程中19例(57.6%)因无法跨越闭塞段及14例(42.4%)因无法重返真腔而进行了REI治疗;行路图下经皮动脉穿刺17例(51.5%),小切口切开直视下穿刺16例(48.5%);手术采用腓动脉入路15例(45.5%),胫后动脉入路11例(33.3%),胫前动脉入路6例(18.2%),腘动脉入路1例(3.0%)。所有患肢均进行了球囊血管成形术,其中REI组3例病人进行了药物涂层球囊血管成形术。REI组仅行球囊血管成形术者(42.0%)少于TFA组(52.0%),而行支架置入者(48.5%)多于TFA组(37.3%),行置管溶栓者(33.3%)也多于TFA组(23.5%),但两组相比较差异均无统计学意义(P>0.05)。
2.2 技术成功率
REI组26例(78.8%)、TFA组92例(90.2%)取得技术成功。REI组的技术失败率相对较高,其中穿刺失败率为18.2%(TFA组穿刺均取得成功),再通失败率为3.0%(TFA组9.8%),但两组比较差异均无统计学意义(P>0.05)。REI组技术失败的7例病人中,6例穿刺失败者(均穿刺腓动脉)在随后的治疗中均穿刺胫前动脉成功,1例因再通失败而行股动脉内膜剥脱+股动脉切开取栓术;而TFA组技术失败的10例病人中,6例仅优化了近端血流,4例行保守治疗。
2.3 手术并发症
REI组病人中,1例术中造影提示远端穿刺血管内血栓形成(术中溶栓治疗后血流恢复),1例足踝部小切口愈合不良,1例小腿部血肿形成,3例病人均不需再次手术治疗。TFA组病人中,3例穿刺部位局限性血肿形成,1例股浅动脉限流性夹层形成(行股浅动脉支架置入术),2例急性股动脉血栓形成(分别行股动脉切开取栓和股动脉内膜剥脱术),1例术中胫前动脉破裂(予以绷带加压)。REI组和TFA组病人手术并发症发生率分别为9.1%和6.9%,两组手术并发症的发生率比较差异无统计学意义(P>0.05)。
2.4 生存率、保肢率和血管通畅率
平均随访19.8个月(1~30月),两组术后30 d均无MAE发生。TFA组和REI组术后1年生存率分别为88.7%和75.7%,术后2年生存率分别为79.6%和59.7%,两组差异均有统计学意义(χ2=4.998,P<0.05)。REI组病人术后1、2年的保肢率分别为93.0%和87.5%,TFA组分别为100.0%和95.4%,两组保肢率比较差异无显著性(P>0.05)。见图2。REI组和TFA组病人的一期通畅率术后1年时分别为48.4%和54.2%,术后2年时分别为29.4%和50.6%;REI组和TFA组的辅助一期通畅率术后1年时分别为63.1%和73.3%,术后2年时分别为36.3%和58.4%。TFA组一期通畅率和辅助一期通畅率虽相对较高,但差异均无统计学意义(P>0.05)。见图3。
3 讨论
随着腔内治疗器材的发展和医师经验的累积,腔内血运重建已经成为股腘动脉闭塞病变治疗的主要方法,特别是对于不能选择外科旁路手术治疗的高风险病人[9-10]。虽然常规经股动脉顺行开通在大多数病人中是可行的,但是仍有10%~20%的复杂CTO病人顺行开通失败,膝下动脉逆行开通则成为一种可行的治疗方案[11-13]。逆行开通更容易跨越病变的原因可能为:斑块的远端纤维帽通常比近端软,这使导丝更容易通过;此外,侧支血管是远端导向的,导丝不易进入侧支血管从而可以避开其干扰;最后,小直径的管腔可能会使导丝和导管有更好的“可控性”[14]。一些研究也证明了REI治疗股腘动脉硬化闭塞疾病的可行性[3,7,15-17]。然而,文献中缺乏膝下动脉REI和常规经股动脉开通的比较报道。
本研究的目的是比较TASCⅡ C/D型股腘动脉硬化闭塞症病人行逆行和顺行开通的短中期效果。结果显示,两组在术后30 d均无MAE发生,TFA组在术后1、2年时的生存率、保肢率、一期通畅率、辅助一期通畅率相对较高,但这与技术操作或穿刺血管并发症无关,而可能与REI组动脉粥样硬化更严重有关[18-19]。本研究中REI组卢瑟福分级5级、6级病变者分别占51.5%和15.2%,而TFA组分别占39.2%和3.0%,两组比较差异有显著性。
REI主要为经股动脉开通治療失败后的补救手段。本研究REI组技术成功率(78.8%)较TFA组(90.2%)低,主要因为REI组有较高的穿刺失败率(18.2%)[20-21]。穿刺失败动脉均为腓动脉,失败可能与腓动脉的环周钙化或严重痉挛有关,但在后面的治疗中均通过穿刺胫前动脉成功开通[14,22-23]。本研究中,REI组和TFA组手术并发症的发生率比较差异无显著性,且REI组仅有1例术中出现远端穿刺血管内血栓形成,术后随访未发现与远端穿刺部位相关的并发症[1,7,16]。为减少远端穿刺部位并发症发生,我们的经验是:使用扩血管药以尽量减少血管痉挛,尽量经股动脉入路进行介入操作(球囊血管成形术或支架置入术),逆行穿刺膝下动脉时尽量不使用导管鞘,且会师成功建立工作轨道后尽早撤出导管。REI组部分采用小切口直视下穿刺,这种技术可以减少血管损伤,尤其是当该血管是膝下流出道唯一的通畅动脉时,但其他并发症如切开可能引起感染和吻合口狭窄值得关注,经皮入路已被证明可以避免组织损伤和灌注不足导致的切口愈合时间延长,因此穿刺方法需视利弊做出选择[24-27]。
综上所述,膝下动脉逆行开通与常规经股动脉开通治疗TASCⅡ C/D型股腘动脉闭塞症,术后短中期的通畅率相当,且远端穿刺部位并发症很少发生,因此REI可作为经股动脉开通失败后的补救治疗手段。但REI治疗的长期效果有待进一步研究。
[参考文献]
[1]RUZSA Z, NEMES B, BNSGHI Z, et al. Transpedal access after failed anterograde recanalization of complex below-the-knee and femoropoliteal occlusions in critical limb ischemia[J]. Catheter Cardiovasc Interventions, 2014,83:997-1007.
[2]NORGREN L, HIATT W R, DORMANDY J A, et al. Inter-society consensus for the management of peripheral arterial disease (TASC Ⅱ)[J]. Journal of Vascular Surgery, 2007,45(1):S5-S67.
[3]LAI S H, FENLON J, ROUSH B B, et al. Analysis of the retrograde tibial artery approach in lower extremity revascula-rization in an office endovascular center[J]. Journal of Vascular Surgery, 2019,70(1):157-165.
[4]HENDRICKS N J, SABRI S S. Subintimal arterial flossing with antegrade-retrograde intervention (SAFARI) and rertograde access for critical limb ischemia[J]. Techniques in Vascular and Interventional Radiology, 2014,17(3):203-210.
[5]RYER E J, ELMORE J R. Commentary: below-the-knee retrograde access for peripheral interventions: a valuable technique for the limb salvage toolbox[J]. Journal of Endovascular Therapy, 2018,25(3):353-354.
[6]SCHMIDT A, BAUSBACK Y, PIORKOWSKI M, et al. Retrograde recanalization technique for use after failed antegrade angioplasty in chronic femoral artery occlusions[J]. Journal of Endovascular Therapy: An Official Journal of the International Society of Endovascular Specialists, 2012,19(1):23-29.
[7]SCHMIDT A, BAKKER O J, BAUSBACK Y, et al. The tibiopedal retrograde vascular access for challenging popliteal and below-the-knee chronic total occlusions: literature review and description of the technique[J]. J Cardiovasc Surg (Torino), 2017,58(3):371-382.
[8]WALKER C M, MUSTAPHA J, ZELLER T, et al. Tibiopedal access for crossing of infrainguinal artery occlusions: a prospective multicenter observational study[J]. Journal of Endovascular Therapy: An Official Journal of the International Society of Endovascular Specialists, 2016,23(6):839-846.
[9]SINGH G D, ARMSTRONG E J, YEO K K, et al. Endovascular recanalization of infrapopliteal occlusions in patients with critical limb ischemia[J]. Journal of Vascular Surgery, 2014,59(5):1300-1307.
[10]MUSTAPHA J A, SAAB F, THERESA M, et al. Tibio-pedal arterial minimally invasive retrograde revascularization in patients with advanced peripheral vascular disease: the TAMI technique, original case series[J]. Catheterization & Cardiovascular Interventions, 2014,83(6):987-994.
[11]SCHEINERT D, BRUNLICH S, SCHEINERT S, et al. Initial clinical experience with an IVUS-guided transmembrane puncture device to facilitate recanalization of total femoral artery occlusions[J]. EuroIntervention, 2005,1(1):115-119.
[12]ADAM D J, BEARD J D, CLEVELAND T. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised, controlled trial[J]. Journal of Vascular Surgery, 2006,44(2):430.
[13]HUA W R, YI M Q, MIN T L, et al. Popliteal versus tibial retrograde access for subintimal arterial flossing with antegrade-retrograde intervention (SAFARI) technique[J]. European Journal of Vascular & Endovascular Surgery, 2013,46(2):249-254.
[14]ROGERS R K, DATTILO P B, GARCIA J A, et al. Retrograde approach to recanalization of complex tibial disease[J]. Catheterization and Cardiovascular Interventions, 2011,77(6):915-925.
[15]WELLING R H A, BAKKER O J, SCHEINERT D, et al. Below-the-knee retrograde access for peripheral interventions: a systematic review[J]. Journal of Endovascular Therapy, 2018,25(3):345-352.
[16]WERNER M, PIORKOWSKI M, SCHMIDT A. Techniques and outcome of retrograde crural artery revascularization[J]. Journal of Cardiovascular Surgery, 2013,54(1 Suppl 1):151-158.
[17]HANNA E B, PROUT D L. Combined radial-pedal access strategy and radial-pedal rendezvous in the revascularization of complex total occlusions of the superficial femoral artery (the “No femoral access” strategy)[J]. Journal of Endovascular Therapy, 2016,23(2):321-329.
[18]WALKER C. Pedal access in critical limb ischemia[J]. J Car-diovasc Surg, 2014,55(2):225-227.
[19]RUTHERFORD R B, BAKER J D, ERNST C, et al. Recommended standards for reports dealing with lower extremity ischemia: revised version[J]. Journal of Vascular Surgery, 1997,26(3):517-538.
[20]MONTERO-BAKER M, SCHMIDT A, BRUNLICH S, et al. Retrograde approach for complex popliteal and tibioperoneal occlusions[J]. Journal of Endovascular Therapy: An Official Journal of the International Society of Endovascular Specia-lists, 2008,15(5):594-604.
[21]EL-SAYED H, BENNETT M E, LOH T M, et al. Retrograde pedal access and endovascular revascularization: a safe and effective technique for high-risk patients with complex ti-bial vessel disease[J]. Annals of Vascular Surgery, 2016,31:91-98.
[22]ABULARRAGE C J, CONRAD M F, HAURANI M J, et al. Long-term outcomes of patients undergoing endovascular infrainguinal interventions with single-vessel peroneal artery runoff[J]. Journal of Vascular Surgery, 2010,52(2):314-22.e1-4.
[23]LICHTENBERG M, KOLKS O, HAILER B, et al. PEACE Ⅰ all-comers registry: patency evaluation after implantation of the 4-French pulsar-18 self-expanding nitinol stent in femoro-popliteal lesions[J]. Journal of Endovascular Therapy, 2014,21(3):373-380.
[24]IYER S S, DORROS G, ZAITOUN R, et al. Retrograde recanalization of an occluded posterior tibial artery by using a posterior tibial cutdown: two case reports[J]. Cathet Cardiovasc Diagn, 1990,20(4):251-253.
[25]AIROLDI F, VITIELLO R, LOSA S, et al. Retrograde recanalization of the anterior tibial artery following surgical vessel exposure: a combined approach for single remaining infragenicular vessel[J]. Journal of Vascular & Interventional Radiology Jvir, 2010,21(6):949-950.
[26]SABRI S S, HENDRICKS N, STONE J, et al. Retrograde pedal access technique for revascularization of infrainguinal arterial occlusive disease[J]. J Vasc Interv Radiol: JVIR, 2015,26(1):29-38.
[27]ZHUANG K D, TAN S G, TAY K H. The “SAFARI” technique using retrograde access via peroneal artery access[J]. CardioVascular and Interventional Radiology, 2012,35(4):927-931.
(本文編辑 马伟平)
- 整合不同教材栏目的设置,提升学生的核心素养
- 关于中小学书法教师校本培训的思考
- 基于核心素养的初中语文整本书阅读教学探究
- 高中生物实验教学中核心素养的培养策略
- 高中音乐教学中学生审美能力的培养
- 基于多元化评价的初中生物课堂教学探究
- 小组合作背景下初中英语读写结合教学探究
- 试析基于核心素养视角下初中历史教学中学生能力的培养
- 基于思维导图的初中语文作文教学探究
- 核心素养下高中数学计算教学研究
- 中考体育训练策略探究
- 浅议心理健康教育在初中语文教学中的渗透
- 浅析初中数学阅读能力培养的重要性
- 高中数学课堂教学师生互动的问题与对策思考
- 核心素养下高中数学情境教学探究
- 核心素养下高中语文群文阅读的开展研究
- 基于核心素养的高中物理实验教学探究
- 基于思维导图的高中地理教学探究
- 高中化学作业设计和实施的策略研究
- 高中物理趣味性教学的应用研究
- 基于核心素养培养的初中语文高效课堂构建初探
- 初中历史教学中学生学习兴趣的有效培养策略分析
- 新课标下初中体育后进生体育学习兴趣培养研究
- 浅谈化学教学中的兴趣激发
- 英语课堂的“国际情”铸就学生未来的“国际心”
- lensed
- lenser
- lensers
- lenses
- lenses'
- lensing
- lensings
- lensless
- lenslet
- lenslike
- lent
- lentil
- lentils
- lents
- leo
- leonian
- leopard
- leopardesses
- leopards
- leo's
- leotard
- leotarded
- leotards
- leper
- lepers
- 感情热烈
- 感情特别专注于某一事物
- 感情特别丰富的人
- 感情状态
- 感情用事
- 感情疏远
- 感情疏远,不亲近
- 感情的强烈度
- 感情的清晰度
- 感情的特殊性
- 感情的自然流露
- 感情真切
- 感情真诚
- 感情真诚恳切
- 感情矢报,日切于中
- 感情破裂
- 感情破裂后又重归于好
- 感情破裂,公开争吵
- 感情破裂,情意断绝
- 感情积累
- 感情移入
- 感情程度
- 感情等不深
- 感情管理
- 感情纠缠不已,不能解脱